1512
Views & Citations512
Likes & Shares
Prostate cancer (PCa) continues to remain most common non-cutaneous malignancy in the United States with a steady increase in incidence in each year. While PSA testing has evolved as a stand-alone diagnostic and prognostic tool over the last decades, there remains a growing need to evaluate newer methods for predicting and evaluating the course of this neoplasm. Few clinical biomarkers specific to cancerous growth have offered some insights into the nature of this disease, Ki67 a nuclear protein finds a special mention in this regard. Ki67 activity often reported as %Ki67 labelling index and is found exaggerated in cancerous cells. We present here findings from our pilot study of 18 patients diagnosed with low to intermediate grade PCa at Moffitt Cancer Center. %Ki67 expression in prostate tissue and adjacent normal tissue was assessed from diagnostic biopsies. %Ki-67 was scored manually by the study pathologist in the tumor cells and adjacent normal-appearing tissue in prepared slides. Cutoff for %Ki67 expression selected at 10% akin to established cut-off in literature. Pilot study comprised of 18 men with average ages 64 (±7.23). Of these, 67% (n=12) diagnosed with GS 6 (3+3) and 33% (n=6) with GS 7 (3+4). Average PSA at diagnosis 7.9 ± 4.8 ng/mL. %Ki67 expression ranged from 0-15 % in patient with GS 6, and 0-16% in patients with GS 7. Acknowledging small sample size as a limitation, our research sets edifice for further research on %Ki67 in well-powered studies. It makes a strong case for need of investigation of this nuclear protein for clinical adoption as a prognostic tool in patients with low to intermediate grade PCa.
Keywords: Ki67, Prostate cancer, PCa, Active surveillance
INTRODUCTION
Prostate cancer (PCa) continues to be the most common non-cutaneous malignancy among men in the United States [1]. In 2020, the American Cancer Society estimated that there will be About 191,930 new cases of prostate cancer in the United States and about 33,330 men will die from this disease [1]. Over the past two decades, PCa detection with serum prostate specific antigen (PSA) has led to a significant increase in the detection of low-grade prostate cancers (Gleason=6), a stage of disease that poses little risk of either metastatic spread or death [2-5]. Currently, the diagnosis of low or intermediate grade PCa is based on clinical (Serum PSA) or histological criteria (number of positive biopsies, percentage of tumor infiltration in these biopsies and histological tumor grade [6-10].
Based on this criterion, studies have demonstrated the indolent nature of low (Gleason 6) and intermediate grade (Gleason 3+4=7) disease, reporting that up to 15% of PSA-detected prostate cancer in white men and up to 37% in black men may have never presented clinically within the patient’s lifetime [11]. Data [10,12] has also suggested that even if untreated, up to 70% of patients with low-grade and 20% of patients with intermediate grade PCa may not experience a clinically relevant disease progression within 15 years, implying that 35% of patients in these groups may be subject to overtreatment [13]. Thus, with a significantly high disease-specific survival for Gleason 6 tumor [14,15] and a significantly lower morbidity [2,4,5,16] Active Surveillance (AS) has been a recommended management strategy for men with low grade disease. However, patient-related challenges such as anxiety, depression, doubts about the possible progression of the disease as well as higher decisional conflict regarding selection of AS [17,18] has led to men on AS ultimately opting for treatment without any key change in clinical diagnosis. Although there are several novel prognostic molecular and genetic biomarkers that continue to be evaluated for clinical utility, specifically to discriminate between insignificant and lethal cancer in the earlier stages of prostate cancer, to date, these biomarkers have not resulted in clinical adoption. The management of these men thus remains controversial [12,19]. Underscoring the need to continue to identify and validate additional prognostic intermediate endpoint biomarkers that are relevant to early and intermediate stage prostate carcinogenesis to sufficiently permit timely therapeutic interventions.
Studies as early as in the 1990s have also explored the prognostic utility of intermediate endpoint biomarkers of proliferation such as %Ki67 expression [20,21]. Immunohistochemistry detection of Ki-67, a nuclear protein, which is expressed in all phases of the cell cycle except the resting G0 phase. The magnitude of its expression has been shown to provide insights into the aggressiveness and the invasiveness of the tumor [22], in addition to the progression of not only aggressive prostate cancers but also the indolent variants [20,23,24]. Ki67 expression has, in addition, been shown to be highly enhanced in prostatic carcinoma and remains low in benign and normal prostatic cells [25,26]. Ki67 labeling index has been demonstrated as an independent predictor of high-grade disease in prostate and other cancers and has been consistently identified as an independent prognostic factor in prostate cancer tissue, and has been corroborated as a negative prognostic factor in PCa. Although a few studies have examined % Ki67 expression in cores positive for PCa in men diagnosed with low or intermediate grade PCa, to date, these studies have not reported data on their observations of % Ki-67 in adjacent normal tissue, data that may inform expression in the tumor microenvironment, relevant in identifying biomarkers for cancer chemoprevention.
The goal of this manuscript is to present results of our pilot data evaluating %Ki67 expression in tumor foci and adjacent normal tissue from the archival prostate biopsy tissue of men diagnosed with low Gleason score 6 (3+3) or intermediate grade PCa (Gleason 7(3+4)) at the Moffitt Cancer Center and managed on active surveillance.
MATERIALS AND METHODS
The study was part of a larger clinical trial, current approved by the institutional review board (Advarra). %Ki67 expression selected for this study was assessed from representative formalin-fixed paraffin-embedded prostate tissue and adjacent normal-appearing tissue obtained from mp-MRI-targeted biopsies in cores positive for prostate cancer, from men on Active Surveillance getting treatment at the Genitourinary Department of Moffitt Cancer Center. The slides were prepared and analyzed by a single Moffitt Cancer Center pathologist. The H&E stained sections were evaluated by light microscopy for presence of cancer by the pathologist and %Ki-67 were scored manually in the tumor cells and adjacent normal-appearing tissue and reported separately for each tissue as average %Ki-67 expression. Cutoff for %Ki67 expression was selected at 10%, akin to what was established by previous research teams [20,27]. Demographic and diagnostic information (like PSA, Gleason Score) of the patients was obtained from their electronic medical record. Descriptive statistics for the study population were generated in Microsoft Excel.
RESULTS AND DISCUSSION
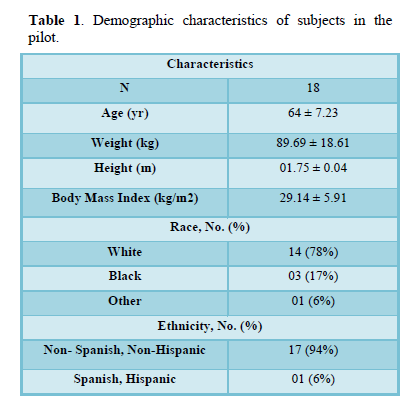
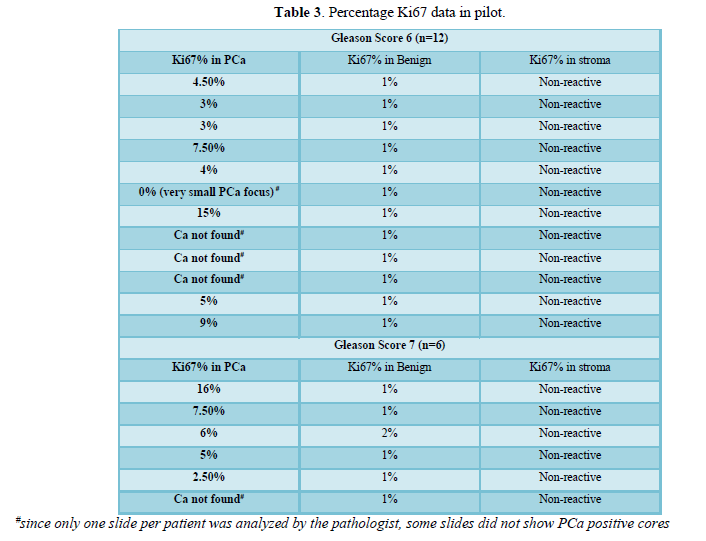
Demographic data of the patient population is summarized (Table 1). The average age of men in this study population was 64 years (±7.23), 78% (n=14) identified as white, 17% (n=3) as black and 6% (n=1) as other. Majority (n=17, 94%) confirmed non-Spanish, non-Hispanic ethnicity. The average BMI for the group was 29.14 (±5.91). Clinical data is presented (Table 2). Of the total 18 patients, 67% (n=12) were diagnosed with GS 6 (3+3) and 33% (n=6) with GS 7 (3+4). The average PSA at diagnosis was 7.9 ± 4.8 ng/mL. Table 3 presents the %Ki-67 expression data. Using a cutoff of %Ki-67 expression of 10[27,20], we observed that among the 12 patients diagnosed with GS 6 (3+3), 91.7% (n=11) had %Ki67 expression <10% and 8.3% (n=1) had %Ki67 expression >10%. The range of %Ki-67 in men with low grade PCa was 0-15%. Of the 6 cases diagnosed with GS 7 (3+4) PCa, 83.3% (n=5) had % Ki67 expression <10% and 16.7% (n=1) had % Ki67 expression >10%. The range of % Ki-67 in this cohort of men with intermediate grade PCa was 0-16%. The %Ki67 expression in the adjacent normal-appearing tissue was 1% for all cases except one where it was 2% where patient had GS 7(3+4) and PCa diagnosis with more than 50% individual biopsy core involvement. The stroma for all cases, however, was non-reactive.
We present here preliminary data of %Ki-67 expression in prostate cancer tissue and adjacent normal tissue for 18 patients who were diagnosed with low Gleason score 6(3+3) or intermediate grade PCa (Gleason 7(3+4)) at the Moffitt Cancer Center and managed on active surveillance. Currently, serum PSA, Gleason score, clinical and pathological tumor staging remain routinely used methods for clinical diagnosis and management of prostate cancer. However, these clinical biomarkers and endpoints require a long-term intervention with agents since PCa has a long latency. Similar to previous studies, %Ki-67 expression in low as well as intermediary risk tumors is greater than adjacent normal.
Studies in the past have consistently observed an exaggeration of %Ki67 expression in cancer cells compared to minimal to none in adjacent normal cells [25,26,28]. However, to our knowledge our review is one of the few to report these findings in tangible numbers.
Similar to previous studies, we observed an enhanced expression of Ki67 in the malignant tissue corroborating the underlying proliferative activity compared to benign adjacent with a normal cell turnover. In their systematic literature review, Carneiro et al [21] documented studies investigating role of Ki67 expression on tissue samples obtained from prostatectomy, biopsy and transurethral resection specimens. Their review demonstrated an association between elevated Ki67 and aggressiveness (p=0.037) as well as shorter tumor-specific survival (p=0.0007). Similar results were reported in a systematic review by [29], where they reviewed 21 studies on localized PCa managed on active surveillance or treated radically and found elevated %Ki67 significantly associated with decreased survival outcomes. They also noted in their review that low %Ki-67 expression tumors showed significantly higher odds of disease-free survival at 5 (OR=0.32, CI=0.23-0.44, p<0.00001) and 10 years (OR=0.31, CI=0.20-0.48, p<0.00001) compared to high %Ki67 expression tumors [23]. Reported their findings from the largest cohort of prostate cancer patients treated conservatively (active surveillance) and showed Ki67 (cut off value 5.42%) staining as a significant prognostic factor for cancer-specific (HR=1.09 (1.07-1.10), p<0.001) and overall survival (HR=1.06 (1.05-1.07), p<0.001). %Ki67 expression was reported as a significant prognostic marker for cancer-specific survival in men with intermediate (p=0.049) and high-risk prostate cancer (p=0.001) by their group [23]. In a follow-up study by their group, they [20] evaluated in the same cohort of conservatively managed men utilizing needle biopsy specimen and showed % Ki67 expression (cut off value 10%) as a significant, independent prognostic marker of prostate cancer death both in univariate (HR=3.42 (1.76, 6.62), χ2 (1 df) =9.8, p=0.0002) and multivariate analysis (HR=2.78 (1.42, 5.46), χ2 (1 df) =7.0, p=0.008) [20]. Additionally, in a study conducted by Nagao et al [30], it was found that % Ki67 expression (cut off value=4.1) levels were significantly valuable in distinguishing clinically significant and insignificant prostate cancers as defined by Epstein and PRIAS criteria. They also reported a significant association between elevated %Ki67 expression and increasing PSA levels (p<0.05) as well with increasing Gleason score (p<0.01) [30]. Their findings corroborated with another study [27], where they had prospectively analyzed needle and radical prostatectomy for a cohort of 279 patients, and reported a significant association between elevated levels of %Ki67 (cut off=10%) expression and advancing tumor stage (p=0.036), lymph node involvement (p<0.001), seminal vesicle infiltration (p<0.001) and large tumor diameter (p=0.039). They reported a significant (p<0.01) prognostic utility of %Ki67 expression in low grade prostate cancers (Gleason score <7), and prostate cancers with only one tissue core positive (p<0.01) [27].
Ki67 labeling index is thus an independent predictor of high-grade disease in prostate and other cancers and has been consistently identified as an independent prognostic factor in prostate cancer, including in localized disease. In addition to the clinical parameters such as serum PSA, volume of tumor and Gleason score, the evaluation of the effectiveness of treatment effectiveness for PCa based on the change in the intermediate biomarkers of proliferation (% Ki-67 expression) in malignant and adjacent normal cells is thus well justified. However, despite an overwhelming evidence supporting the prognostic utility of Ki67 expression in predicting the course of PCa, there remains a lack of clinical adoption of the same [10,28]. This lack in translation has largely been attributed to incongruity on cut-off values [10,31], especially in low to intermediate grade PCa. As our study population solely comprised of men with low to intermediate grade PCa, the majority (n=16) in our study population showed %Ki67 expression <10%. The two cases with %Ki67 expression >10% also showed an extensive individual core involvement (>50%), similar to findings reported in the literature, where higher %Ki67 expression is reported in more aggressive disease. Additionally, we observed Ki67 expression at 2% in benign and 6% in malignant tissue despite a low-grade Gleason score (GS 6). However, the percentage involvement of individual cores for this case remained high (>50%) similar to the cases with intermediate risk. These observations establish the need to continue to further identify and validate non-clinical prognostic factors in addition to clinical markers for PCa in well powered studies.
The major limitation to our study is that it was a pilot study with a small sample size. Thus, these results need further validation in well powered studies. Second, our study utilized a random single slide from 12 core biopsies for each of these subjects which may have contributed to some underrepresentation of %Ki67 expression, based on the sampling. However, we have compared our findings to what is reported in the literature and set a foundation for further investigation and validation of this biomarker in both the cancer tissue as well as the adjacent normal.
CONCLUSION
We report here early findings of % Ki67 expression in cores positive for PCa in addition to adjacent normal tissue in men diagnosed with low or intermediate grade PCa. Although the study was a pilot trial and not well powered, the data demonstrates congruence to previous data in the literature. Additionally, our data underscores the need to continue to examine Ki-67 expression in cancer and adjacent normal tissue or in the tumor microenvironment, relevant in evaluating efficacy of agents in chemoprevention and treatment.
ACKNOWLEDGMENT
The authors thank Alyse Johnson for her assistance with this manuscript.
FUNDING
The study was funded by the National Cancer Institute R01CA235032-02.
CONFLICT OF INTERESTS
The author(s) declared no conflict of interests.
1. Key Statistics for Prostate cancer (2019) Available online at : http://www.cancer.org/Cancer/ProstateCancer/DetailedGuide/prostate-cancer-key-statistics
2. Bruinsma SM, Bangma CH, Carroll PR, Leapman MS, Rannikko A, et al. (2016) Active surveillance for prostate cancer : A narrative review of clinical guidelines. Nat Rev Urol 13 : 151-167.
3. Stanley IP, Dahabreh IJ, Chung M, Winifred WY, Balk EM, et al. (2011) An evidence review of active surveillance in men with localized prostate cancer. Evid Rep Technol Assess 204 : 1-341.
4. Klotz L (2005) Active surveillance for prostate cancer : For whom? J Clin Oncol 23 : 8165-8169.
5. Thompson I, Thrasher JB, Aus G, Burnett AL, Canby-Hagino ED, et al. (2007) Guideline for the management of clinically localized prostate cancer : 2007 updates. J Urol 177 : 2106-2131.
6. Dall'Era MA, Cooperberg MR, Chan JM, Davies BJ, Albertsen PC, et al. (2008) Active surveillance for early-stage prostate cancer : Review of the current literature. Cancer 112 :1650-1659.
7. Harnden P, Naylor B, Shelley MD, Clements H, Coles B, et al. (2008) The clinical management of patients with a small volume of prostatic cancer on biopsy: What are the risks of progression? A systematic review and meta-analysis. Cancer 112 : 971-981.
8. Klotz L (2007) Active surveillance for favorable risk prostate cancer : rationale, risks, and results. Urol Oncol 25 : 505-509.
9. Loeb S, Roehl KA, Thaxton CS, Catalona WJ (2008) Combined prostate-specific antigen density and biopsy features to predict “clinically insignificant” prostate cancer. Urology 72 : 143-147.
10. Kristiansen G (2012) Diagnostic and prognostic molecular biomarkers for prostate cancer. Histopathology 60 : 125-141.
11. Harlan SR, Cooperberg MR, Elkin E, Lubeck DP, Meng MV, et al. (2003) Time trends and characteristics of men choosing watchful waiting for initial treatment of localized prostate cancer : Results from CaPSURE. J Urol 170 : 1804-1807.
12. Albertsen PC, Hanley JA, Gleason DF, Barry MJ (1998) Competing risk analysis of men aged 55 to 74 years at diagnosis managed conservatively for clinically localized prostate cancer. JAMA 280 : 975-980.
13. Lein M, Stibane I, Mansour R, Hege C, Roigas J, et al. (2006) Complications, urinary continence and oncologic outcome of 1000 laparoscopic transperitoneal radical prostatectomies-experience at the Charité Hospital Berlin, Campus Mitte. Eur Urol 50 :1278-1282.
14. Klotz L, Zhang L, Lam A, Nam R, Mamedov A, et al. (2010) Clinical results of long-term follow-up of a large, active surveillance cohort with localized prostate cancer. J Clin Oncol 28 : 126-131.
15. Klotz L (2015) Active surveillance for low-risk prostate cancer. Curr Urol Rep 16 : 24.
16. Hamdy FC, Donovan JL, Neal DE (2017) 10-Year Outcomes in Localized Prostate Cancer. N Engl J Med 376 : 180.
17. Cooperberg MR, Carroll PR (2015) Trends in management for patients with localized prostate cancer, 1990-2013. JAMA 314 : 80-82.
18. Orom H, Underwood W, Biddle C (2017) Emotional distress increases the likelihood of undergoing surgery among men with localized prostate cancer. J Urol 197 : 350-355.
19. Chodak GW, Thisted RA, Gerber GS, Johansson JE, Adolfsson J, et al. (1994) Results of conservative management of clinically localized prostate cancer. N Engl J Med 330 : 242-248.
20. Fisher G, Yang ZH, Kudahetti S, Møller H, Scardino P, et al. (2013) Prognostic value of Ki-67 for prostate cancer death in a conservatively managed cohort. Br J Cancer 108 : 271-277.
21. Carneiro A, Barbosa ÁRG, Takemura LS, Kayano PP, Moran NKS, et al. (2018) The role of immunohistochemical analysis as a tool for the diagnosis, prognostic evaluation and treatment of prostate cancer : A systematic review of the literature. Front Oncol 8 : 377.
22. Mohamed AA, Abbas MY, Alharbi H, Babiker AY (2018) Assessment of expression of Ki-67 in Benign and malignant prostatic lesions among Sudanese patients. Open Access Maced J Med Sci 6 : 1809-1812.
23. Berney DM, Gopalan A, Kudahetti S, Fisher G, Ambroisine L, et al. (2009) Ki-67 and outcome in clinically localised prostate cancer : Analysis of conservatively treated prostate cancer patients from the Trans-Atlantic Prostate Group study. Br J Cancer 100 : 888-893.
24. Jhavar S, Bartlett J, Kovacs G, Corbishley C, Dearnaley D, et al. (2009) Biopsy tissue microarray study of Ki-67 expression in untreated, localized prostate cancer managed by active surveillance. Prostate Cancer Prostatic Dis 12 : 143-147.
25. Guertin MH, Robitaille K, Pelletier JF, Duchesne T, Pierre Julien, et al. (2018) Effects of concentrated long-chain omega-3 polyunsaturated fatty acid supplementation before radical prostatectomy on prostate cancer proliferation, inflammation and quality of life : Study protocol for a phase IIb, randomized, double-blind, placebo-controlled trial. BMC Cancer 18 : 64.
26. Grover SK, Agarwal S, Gupta S, Wadhwa N, Sharma N (2015) Expression of estrogen receptor β and Ki 67 in benign & malignant human prostate lesions by immunohistochemistry. Pathol Oncol Res 21 : 651-657.
27. Zellweger T, Günther S, Zlobec I, Savic S, Sauter G, et al. (2009) Tumor growth fraction measured by immunohistochemical staining of Ki67 is an independent prognostic factor in preoperative prostate biopsies with small-volume or low-grade prostate cancer. Int J Cancer 124 : 2116-2123.
28. Li LT, Jiang G, Chen Q, Zheng JN (2015) Ki67 is a promising molecular target in the diagnosis of cancer (review). Mol Med Rep 11 : 1566-1572.
29. Berlin A, Castro-Mesta JF, Rodriguez-Romo L, Hernandez-Barajas D, González-Guerrero JF, et al. (2017) Prognostic role of Ki-67 score in localized prostate cancer : A systematic review and meta-analysis. Urol Oncol 35 : 499-506.
30. Nagao K, Yamamoto Y, Hara T, Komatsu H, Inoue R, et al. (2011) Ki67 and BUBR1 may discriminate clinically insignificant prostate cancer in the PSA range
31. Lobo J, Rodrigues Â, Antunes L, GraçaI, Ramalho-Carvalho J, et al. (2018) High immunoexpression of Ki67, EZH2 and SMYD3 in diagnostic prostate biopsies independently predicts outcome in patients with prostate cancer. Urol Oncol 36 : 161.e167-161.e117.
-
 Table 1
Table 1 -
Table 2
-
Table 3

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- International Journal of Diabetes (ISSN: 2644-3031)
- BioMed Research Journal (ISSN:2578-8892)
- Chemotherapy Research Journal (ISSN:2642-0236)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)


